3. Disaster Response
In 2006, Latin Americ and the Caribbean were spared major disasters
of the magnitude of Tropical Storm Stan (2005) or Hurricane Ivan
(2004). However, many other emergency situations posed serious
concerns and required substantial technical support from PAHO/WHO.
A review of these situations in which PAHO worked with member
states to respond to pressing health issues is provided below.

 Unusually
high seasonal rainfall at the end of 2005 caused widespread flooding
in several Regions of Guyana
in early 2006. The government declared Regions 2 (Pomeroon/Supenaam)
and 5 (Mahaica/Berbice) as disaster areas and an international
appeal was launched to secure support and assistance. PAHO/WHO
worked with the Ministry of Health to conduct disease surveillance
and manage health and environmental issues in the shelters. Medical
teams from the Ministry worked closely with the Civil Defense
Commission and in the flooded areas to deliver health care daily.
There was an increase in the number of persons admitted to the
Georgetown Public Hospital with a suspected diagnosis of leptospirosis.
The appropriate treatment, prophylactic doxycycline, was administered
in the flooded areas and in other areas where cases were detected.
Unusually
high seasonal rainfall at the end of 2005 caused widespread flooding
in several Regions of Guyana
in early 2006. The government declared Regions 2 (Pomeroon/Supenaam)
and 5 (Mahaica/Berbice) as disaster areas and an international
appeal was launched to secure support and assistance. PAHO/WHO
worked with the Ministry of Health to conduct disease surveillance
and manage health and environmental issues in the shelters. Medical
teams from the Ministry worked closely with the Civil Defense
Commission and in the flooded areas to deliver health care daily.
There was an increase in the number of persons admitted to the
Georgetown Public Hospital with a suspected diagnosis of leptospirosis.
The appropriate treatment, prophylactic doxycycline, was administered
in the flooded areas and in other areas where cases were detected.
 Virtually
every year, Bolivia
experiences a cyclical pattern of intense rainfall, hail, mudslides
and floods. In the early months of 2006, major rivers overflowed
and the rains triggered landslides and obstructed roads, isolating
some communities. The most affected departments included Santa
Cruz, Beni, Cochabamba, Trinidad, Pando, Potosi and La Paz. A
population of 200,000 was affected and 21,000 were left homeless
and were housed in shelters. Although there was no major damage
to health services, the number of cases of respiratory and digestive
illnesses and conjunctivitis rose among the population in shelters.
Local health authorities managed the situation. The health thematic
group, led by PAHO/ WHO in coordination with the Ministry of Health,
stepped up epidemiological surveillance, vector control and vaccinations
and assessed the need for medicines. The supply management system
(LSS/SUMA) was used to manage donations.
Virtually
every year, Bolivia
experiences a cyclical pattern of intense rainfall, hail, mudslides
and floods. In the early months of 2006, major rivers overflowed
and the rains triggered landslides and obstructed roads, isolating
some communities. The most affected departments included Santa
Cruz, Beni, Cochabamba, Trinidad, Pando, Potosi and La Paz. A
population of 200,000 was affected and 21,000 were left homeless
and were housed in shelters. Although there was no major damage
to health services, the number of cases of respiratory and digestive
illnesses and conjunctivitis rose among the population in shelters.
Local health authorities managed the situation. The health thematic
group, led by PAHO/ WHO in coordination with the Ministry of Health,
stepped up epidemiological surveillance, vector control and vaccinations
and assessed the need for medicines. The supply management system
(LSS/SUMA) was used to manage donations.
 Along
Ecuador’s
Pacific coast, rainfall that began in January caused major flooding
and affected 150,000 persons in six coastal provinces (29,115
families). More than 1,100 families were evacuated to shelters
(schools and other municipal buildings that were improvised for
this purpose). The MoH and PAHO/WHO focused on activating emergency
operations centers; the assessment of damage and needs; vector
control (spraying and fumigation); mobilizing medical brigades
to provide health services to the population in flooded areas
of the country; stocking health facilities with medicines and
delivering safe drinking water and chlorine for water treatment
in affected communities. International aid was mobilized to improve
public health measures and reduce the risk of communicable diseases.
The result was that the outbreaks were controlled, thanks to surveillance,
detection and opportune treatment; access was improved to safe
water and sanitation; and appropriate community actions were taken
to control vectors.
Along
Ecuador’s
Pacific coast, rainfall that began in January caused major flooding
and affected 150,000 persons in six coastal provinces (29,115
families). More than 1,100 families were evacuated to shelters
(schools and other municipal buildings that were improvised for
this purpose). The MoH and PAHO/WHO focused on activating emergency
operations centers; the assessment of damage and needs; vector
control (spraying and fumigation); mobilizing medical brigades
to provide health services to the population in flooded areas
of the country; stocking health facilities with medicines and
delivering safe drinking water and chlorine for water treatment
in affected communities. International aid was mobilized to improve
public health measures and reduce the risk of communicable diseases.
The result was that the outbreaks were controlled, thanks to surveillance,
detection and opportune treatment; access was improved to safe
water and sanitation; and appropriate community actions were taken
to control vectors.
 The
department of Nariño, Colombia
was put on high alert when seismic activity increased around the
Galeras volcano (which had been active again since mid-2004) and
the alert level was raised to level II. The volcano threatened
seven municipalities with a population of almost 8,000. The population
closest to the volcano—some 2,500 people—was evacuated
to shelters. Health facilities in the at-risk area were also put
on alert and hospital emergency and contingency plans were activated
for a potential volcanic eruption. Some health programs in the
area were interrupted because the level of staffing decreased.
PAHO/WHO supported the departmental and municipal health authorities
by designing clean, healthy temporary shelters and a module for
triage and stabilization of the injured. The Organization also
supported other public health actions, including psychosocial
and mental health support and communications. A simulation exercise
was carried out, a health crisis situation room set up and the
LSS/SUMA system was put in place to manage humanitarian aid.
The
department of Nariño, Colombia
was put on high alert when seismic activity increased around the
Galeras volcano (which had been active again since mid-2004) and
the alert level was raised to level II. The volcano threatened
seven municipalities with a population of almost 8,000. The population
closest to the volcano—some 2,500 people—was evacuated
to shelters. Health facilities in the at-risk area were also put
on alert and hospital emergency and contingency plans were activated
for a potential volcanic eruption. Some health programs in the
area were interrupted because the level of staffing decreased.
PAHO/WHO supported the departmental and municipal health authorities
by designing clean, healthy temporary shelters and a module for
triage and stabilization of the injured. The Organization also
supported other public health actions, including psychosocial
and mental health support and communications. A simulation exercise
was carried out, a health crisis situation room set up and the
LSS/SUMA system was put in place to manage humanitarian aid.
 Following
torrential rains in May, Suriname
declared the southern region of the country a disaster area and
requested international assistance. PAHO/ WHO deployed five experts
to support the Country Office to assess health needs and mobilize
resources. A Supply Management team was also deployed and the
LSS/SUMA system put in place. A sanitary engineer, already on
the ground, provided technical support. Experience has shown that
in this region of the country, flooding is generally followed
by malaria outbreaks. Therefore, PAHO/WHO procured and distributed
insecticide-impregnated bed nets and malaria testing kits and
conducted training on the use of the latter. Water tanks were
installed in affected communities to allow the population to collect
rain water and thus prevent outbreaks of diarrheal disease. PAHO/WHO
held a lessons learned exercise and began developing a contingency
plan for the health sector, as Suriname did not have one.
Following
torrential rains in May, Suriname
declared the southern region of the country a disaster area and
requested international assistance. PAHO/ WHO deployed five experts
to support the Country Office to assess health needs and mobilize
resources. A Supply Management team was also deployed and the
LSS/SUMA system put in place. A sanitary engineer, already on
the ground, provided technical support. Experience has shown that
in this region of the country, flooding is generally followed
by malaria outbreaks. Therefore, PAHO/WHO procured and distributed
insecticide-impregnated bed nets and malaria testing kits and
conducted training on the use of the latter. Water tanks were
installed in affected communities to allow the population to collect
rain water and thus prevent outbreaks of diarrheal disease. PAHO/WHO
held a lessons learned exercise and began developing a contingency
plan for the health sector, as Suriname did not have one.
 The
Tungurahua volcano in Ecuador
has been active for the last six years and in mid-2006 eruptions
killed five persons and affected almost 450,000 in the provinces
of Tungurahua and Chimborazo (to put this in perspective, the
total population of these provinces is 915,588). In the high-risk
areas, more than 14,000 people were evacuated either to shelters
or to the homes of family or friends. Many of these families returned
home once the level of volcanic activity diminished, however,
these was a substantial impact on health centers, agriculture
and livestock and mudflows destroyed homes. In the affected provinces
medical teams were deployed to shelters and regular follow up
was conducted through a health situation room. The LSS/SUMA system
was set up in both affected provinces to manage humanitarian aid.
Months later, some 2,500 persons from five communities in the
most at-risk area still remained in temporary shelters pending
the relocation of their homes to safer sites.
The
Tungurahua volcano in Ecuador
has been active for the last six years and in mid-2006 eruptions
killed five persons and affected almost 450,000 in the provinces
of Tungurahua and Chimborazo (to put this in perspective, the
total population of these provinces is 915,588). In the high-risk
areas, more than 14,000 people were evacuated either to shelters
or to the homes of family or friends. Many of these families returned
home once the level of volcanic activity diminished, however,
these was a substantial impact on health centers, agriculture
and livestock and mudflows destroyed homes. In the affected provinces
medical teams were deployed to shelters and regular follow up
was conducted through a health situation room. The LSS/SUMA system
was set up in both affected provinces to manage humanitarian aid.
Months later, some 2,500 persons from five communities in the
most at-risk area still remained in temporary shelters pending
the relocation of their homes to safer sites.
 In
Haiti, heavy rains
caused by Hurricane Ernesto in August hit the coastal areas of
the departments of Sud, Sud-est, Ouest, Grand-Anse, L’Artibonite,
and the Northwest; however, no major flooding or significant damage
to infrastructure were reported. Two people died and 200 had to
be evacuated. Nineteen houses were destroyed and 134 damaged.
Several localities in Port-au-Prince (Martissant, Gressier and
Mariani) along southbound roads were flooded. WHO/PAHO pre-positioned
essential medicines (kit 10,000) in Port-au-Prince (2), Le Cayes
(2) and Jeremie (1).
In
Haiti, heavy rains
caused by Hurricane Ernesto in August hit the coastal areas of
the departments of Sud, Sud-est, Ouest, Grand-Anse, L’Artibonite,
and the Northwest; however, no major flooding or significant damage
to infrastructure were reported. Two people died and 200 had to
be evacuated. Nineteen houses were destroyed and 134 damaged.
Several localities in Port-au-Prince (Martissant, Gressier and
Mariani) along southbound roads were flooded. WHO/PAHO pre-positioned
essential medicines (kit 10,000) in Port-au-Prince (2), Le Cayes
(2) and Jeremie (1).
 In
early October, the Chaparrastique volcano, near the town of San
Miguel, El Salvador,
began to show increasing signs of activity. Prompted by this threat,
the disaster office of the Ministry of Health organized training
sessions for health personnel on damage and needs assessment.
These workshops which took on a more realistic character, given
the risk conditions in the area. The health sector was encouraged
to step up coordination with other sectors, particularly the municipal
civil protection system; a health emergency committee was organized
and made operational. Health and environmental conditions in the
Isidro Menendez Institute, which had been designated as an emergency
shelter were evaluated and a stock of medial supplies was replenished
in the at-risk area.
In
early October, the Chaparrastique volcano, near the town of San
Miguel, El Salvador,
began to show increasing signs of activity. Prompted by this threat,
the disaster office of the Ministry of Health organized training
sessions for health personnel on damage and needs assessment.
These workshops which took on a more realistic character, given
the risk conditions in the area. The health sector was encouraged
to step up coordination with other sectors, particularly the municipal
civil protection system; a health emergency committee was organized
and made operational. Health and environmental conditions in the
Isidro Menendez Institute, which had been designated as an emergency
shelter were evaluated and a stock of medial supplies was replenished
in the at-risk area.
 In
late November, Haiti
once again experienced extreme weather due to a cold front in
several parts of the country. The unusually heavy rainfall caused
serious flooding in Grande-Anse and in the North-West region.
Seven persons died and more than 4,000 families were directly
affected. At least 335 persons were temporarily sheltered in Jeremie
(Grand Anse). Two hospitals and their pharmacies, which were already
in precarious conditions, were flooded, severely affecting the
population at large. PAHO took the lead in coordinating the health
response, and together with the Ministry of Health, pre-positioned
medicines and distributed medical supplies to the health sector
in the affected areas, either to replace the losses or to strengthen
the capacity to treat the injured and ill. An emergency assessment
showed that eight potable water distribution systems were destroyed
or severely damaged in Grand Anse and Nord-Ouest. PAHO/WHO coordinated
with partners on the ground to facilitate distribution of water
while repairs were made to the affected water systems.
In
late November, Haiti
once again experienced extreme weather due to a cold front in
several parts of the country. The unusually heavy rainfall caused
serious flooding in Grande-Anse and in the North-West region.
Seven persons died and more than 4,000 families were directly
affected. At least 335 persons were temporarily sheltered in Jeremie
(Grand Anse). Two hospitals and their pharmacies, which were already
in precarious conditions, were flooded, severely affecting the
population at large. PAHO took the lead in coordinating the health
response, and together with the Ministry of Health, pre-positioned
medicines and distributed medical supplies to the health sector
in the affected areas, either to replace the losses or to strengthen
the capacity to treat the injured and ill. An emergency assessment
showed that eight potable water distribution systems were destroyed
or severely damaged in Grand Anse and Nord-Ouest. PAHO/WHO coordinated
with partners on the ground to facilitate distribution of water
while repairs were made to the affected water systems.
 In
the latter part of November, intense rainfall devastated much
of Panama, leaving
11 dead and 1,300 displaced persons that required support from
local authorities. Five health facilities were damaged (one health
center and four health posts which provide only primary care).
The disaster office of the Ministry of Health coordinated the
sector’s response. PAHO/WHO coordinated the assessment of
damage to health facilities and helped to set up a health situation
room for information analysis both in Panama City (the capital)
and in the affected departments. Working together with the UN
Emergency Team, national authorities in Panama initiated the use
of a single form to capture information on an ongoing basis. As
a result, authorities determined that no external aid was required,
although neighboring countries provided some donations.
In
the latter part of November, intense rainfall devastated much
of Panama, leaving
11 dead and 1,300 displaced persons that required support from
local authorities. Five health facilities were damaged (one health
center and four health posts which provide only primary care).
The disaster office of the Ministry of Health coordinated the
sector’s response. PAHO/WHO coordinated the assessment of
damage to health facilities and helped to set up a health situation
room for information analysis both in Panama City (the capital)
and in the affected departments. Working together with the UN
Emergency Team, national authorities in Panama initiated the use
of a single form to capture information on an ongoing basis. As
a result, authorities determined that no external aid was required,
although neighboring countries provided some donations.
Other Health Crises
 Forty-eight
persons died and 15 were blinded by the toxic effects of methanol
in an incident of mass poisoning in Nicaragua.
Between 2-20 September, 801 people were treated for methanol poisoning
following the ingestion of home-brewed local alcohol known as
“guaro,” which had been contaminated by methanol.
Most cases occurred in the departments of León and Chinandega.
Forty-eight
persons died and 15 were blinded by the toxic effects of methanol
in an incident of mass poisoning in Nicaragua.
Between 2-20 September, 801 people were treated for methanol poisoning
following the ingestion of home-brewed local alcohol known as
“guaro,” which had been contaminated by methanol.
Most cases occurred in the departments of León and Chinandega.
The Network of Toxicology of Latin America and the Caribbean
(RETOXLAC) played a critical role by providing information to
Nicaragua’s Toxicology Reference Center on case management,
identifying a new antidote and making a network member available
for on-site technical assistance. A U.S. drug company, Jazz Pharmaceuticals,
donated the antidote medicine—1,200 vials were delivered
to Nicaragua and put to immediate use.
PAHO/WHO’s role included identifying experts to review
protocols for poisoned patients; coordinating the health response
and implementing contingency plans. It also organized epidemiological
surveillance at the local and national level, and supported the
Ministry of Health in active case detection at the grass roots
level by helping to train 533 Nicaraguan health staff. PAHO/WHO
also assisted in the coordination and management of the donation
and importation of the antidote (Fomepizole) and the local purchase
of other essential drugs and supplies.
In
Panama, 91 patients
suffered acute renal insufficiency syndrome caused by the accidental
ingestion of cough syrup contaminated with diethylenglycol (DEG).
Forty-five people died and some patients who received treatment
were left in critical condition. A national campaign was launched
to identify the causal agent, ensure that patients received medical
treatment and destroy the adulterated medicines. PAHO/WHO assisted
the Ministry of Health in the investigation and control of the
outbreak, with the help of international experts in epidemiology,
toxicology, and communications. Once the diethylenglycol was identified,
PAHO/WHO also helped to acquire the recommended antidote (Fomepizol)
and the clinical support for its use.
Complex Emergencies
Haiti
 In
2006, PAHO/WHO coordinated the installation of two Emergency Operation
Centers in Les Cayes and Jacmel. Equipping these centers and staff
with computers, satellite Internet access and other office equipment
allowed them to play a more active role in managing disaster alerts,
evaluating needs and responding to natural disasters.
In
2006, PAHO/WHO coordinated the installation of two Emergency Operation
Centers in Les Cayes and Jacmel. Equipping these centers and staff
with computers, satellite Internet access and other office equipment
allowed them to play a more active role in managing disaster alerts,
evaluating needs and responding to natural disasters.
PAHO/WHO supported the participation of three Haitian medical
doctors (trainers in mass casualty management) in a regional training
in Martinique and Guadeloupe, organized by the University of Bordeaux,
France. The purpose of their participation was to improve their
technical capacity to review the existing curriculum in Haiti
and develop new training materials and workshops. Subsequently,
several specialized courses/activities were carried out:

-
 In
March, emergency room personnel (30 people) from the department
of Sud were trained in the management of medical/surgical cases.
The same course was replicated in Jacmel, Sud-est department
in June.
In
March, emergency room personnel (30 people) from the department
of Sud were trained in the management of medical/surgical cases.
The same course was replicated in Jacmel, Sud-est department
in June.
- Thirty first responders (police, fire brigade,
Red Cross volunteers, hospital staff, etc.) were trained in
mass casualty management in May. In addition to practical training
on health contingency planning, mass casualty management, psycho-social
care, epidemiological surveillance and humanitarian supply management,
two simulation exercises were carried out. The course was repeated
in another department in June.
- Haiti’s Civil Defense (DPC) carried out
courses in general disaster management and contingency planning
in April. These courses were the result of joint efforts between
PAHO/WHO and UNDP to ensure that the departments had improved
and updated contingency plans for disaster management at departmental
level. In May, the department of Sud-est finalized and disseminated
its plan; the department of Sud finished its plan in August.
Both plans were used for Hurricane Ernesto and the departments
agreed to evaluate them to determine future needs for disaster
preparedness at departmental level.
Prior to the start of hurricane season, shelters (churches and
schools) in isolated areas were prestocked with supplies and the
Local Disaster Committees in the Departments of Sud and Sud-est
received other material support to conduct minor infrastructure
repairs. Local Disaster Committees also were outfitted with vests
and caps to properly identify community and departmental Committee
members. When health facilities and services were affected by
flooding, PAHO/WHO supported the public health system with essential
medicines and supplies. In 2006, six WHO Emergency Health Kits
were distributed throughout Haiti, enabling a population of 60,000
to be treated over a three-month period.
Colombia
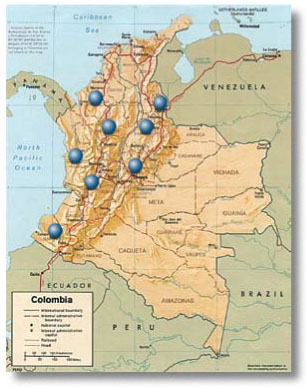 PAHO/WHO
continued to provide technical cooperation to health authorities
in Colombia to improve access to health care for the internally
displaced population (IDPs), the vulnerable population in the
receptor communities and refugees crossing borders from neighboring
countries. In 2006, PAHO/WHO managed these activities through
eight field offices in Nariño, Valle, Chocó, Cordoba,
Norte de Santander, Santander, Antioquia and Cundinamarca. The
IDP target population in these departments is 732,000 persons.
PAHO/WHO
continued to provide technical cooperation to health authorities
in Colombia to improve access to health care for the internally
displaced population (IDPs), the vulnerable population in the
receptor communities and refugees crossing borders from neighboring
countries. In 2006, PAHO/WHO managed these activities through
eight field offices in Nariño, Valle, Chocó, Cordoba,
Norte de Santander, Santander, Antioquia and Cundinamarca. The
IDP target population in these departments is 732,000 persons.
By including the variable “displaced” in data collection
surveys, health information and statistics on IDPs was improved.
This allowed health authorities to better plan and execute specific
programs. Nationally, funding was increased for health care and
health promotion programs for the displaced population. Some of
the specific achievements of 2006 include:
- In Valle, the SIGA software was field tested
and used to track the execution of funds earmarked for health
expenditures for IDPs. Set up in hospitals that provide health
care to IDPs, the software collected information on their health
status and prevalent diseases, medical procedures performed
and the cost of treatment. Hospitals reported this information
to the Departmental health authorities and to the Ministry of
Social Protection. This previously uncollected information was
used to track the use of allocated funds, determine the number
of beneficiaries, and plan specific interventions according
to the epidemiological information available. It yielded morbidity
and mortality data, disaggregated by gender, age, ethnicity
and disability. The Colombian Ministry of Social Protection
will now use this software at thenational level.
- PAHO/WHO supported the publication, by local
health authorities, of basic health indicators on IDPs. In Nariño
and Santander, a web site on health and displacement was created
and local and national health authorities, UN agencies, NGOs
and othersare using the information to plan and follow up specific
health programs.
-
 The
web site on Health and Displacement (created and managed by
the PAHO/WHO Representation in Bogotá) continues to publish
technical information and reports on health and displacement
and emergency situations. The site, used by national and international
institutions, NGOs, universities, and others, received 1.2 million
hits in 2006. The site has improved collaboration among institutions,
as it provides open access to studies, official statistics,
NGO and UN information and links to other national and international
sources on IDP health issues. See Annex 10 for the homepage
of this website. (www.disaster-info.net/desplazados)
The
web site on Health and Displacement (created and managed by
the PAHO/WHO Representation in Bogotá) continues to publish
technical information and reports on health and displacement
and emergency situations. The site, used by national and international
institutions, NGOs, universities, and others, received 1.2 million
hits in 2006. The site has improved collaboration among institutions,
as it provides open access to studies, official statistics,
NGO and UN information and links to other national and international
sources on IDP health issues. See Annex 10 for the homepage
of this website. (www.disaster-info.net/desplazados)
- PAHO/WHO collaborated in epidemiological surveillance
efforts along the Colombia-Ecuador border to identify 35 common
diseases and to develop a software application to analyze the
health situation in border municipalities. This software will
collect health information from official sources at the departmental,
municipal and national levels and compile updated health information
to improve decision making. The system will also improve municipal-level
health surveillance and will be implemented in 2007.
- The allocation of funding for IDP health issues
and the execution of projects improved at the departmental level
in Santander, Valle, Cundinamarca and Cordoba. PAHO´s
technical cooperation allowed health authorities to identify,
access and manage specific national resources earmarked for
IDP health care, of which they were formerly unaware. As a result,
health authorities were able to integrate resources for health
promotion, disease prevention and treatment into the local health
budget (previously, resources earmarked for the poor rather
than for IDPs were used).
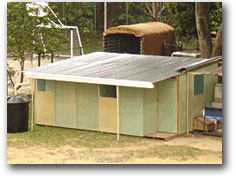 The “Healthy Homes” initiative was implemented in
all Departments where PAHO has field offices. It aims to improve
household conditions related to water quality, sanitation, refuse,
food, and animals. National and local authorities, UN agencies,
the private sector and NGOs worked together to implement and
follow up the initiative. Demonstration projects were implemented
in Nariño, Chocó, Santander and Norte de Santander
as a low-cost solution that is quick to install and easily transportable
for displaced population. It includes a toilet, clothes washing
areas, a shower, domestic water filters, separate bedrooms for
children and adults, kitchen, dining table and seats, trash
container, closet, solar oven, and a rain water collection system.
This home will help resolve some of the most pressing needs
for shelter and sanitation for those who have lost their homes
due to displacement and/or natural disasters. PAHO/WHO designed
and installed the Healthy Home Family Shelter model with input
of universities and IDPs.
The “Healthy Homes” initiative was implemented in
all Departments where PAHO has field offices. It aims to improve
household conditions related to water quality, sanitation, refuse,
food, and animals. National and local authorities, UN agencies,
the private sector and NGOs worked together to implement and
follow up the initiative. Demonstration projects were implemented
in Nariño, Chocó, Santander and Norte de Santander
as a low-cost solution that is quick to install and easily transportable
for displaced population. It includes a toilet, clothes washing
areas, a shower, domestic water filters, separate bedrooms for
children and adults, kitchen, dining table and seats, trash
container, closet, solar oven, and a rain water collection system.
This home will help resolve some of the most pressing needs
for shelter and sanitation for those who have lost their homes
due to displacement and/or natural disasters. PAHO/WHO designed
and installed the Healthy Home Family Shelter model with input
of universities and IDPs.
The areas of Colombia with the greatest population of IDPs were
also the site of floods and landslides in 2006. PAHO/WHO worked
with national and local authorities in those departments to coordinate
the primary health response, conduct epidemiological surveillance,
implement basic sanitary measures in temporary shelters, provide
psychosocial aid to the affected population and evaluate damage
to health facilities. As a result, preventive emergency measures
and surveillance systems helped avoid public health problems in
flood-affected areas.
Regional Health Disaster Response Team
In response to the vulnerability of Latin America and the Caribbean
to major sudden-impact disasters— some of which strike multiple
countries at the same time, as was the case with Hurricane Mitch
in Central America—preparations went forward to ensure that
the PAHO/WHO Health Disaster Response Team is ready for deployment
in emergency situations.
Training
The initial identification and selection of team members was
completed and to date, 80 team members have been selected from
among PAHO’s professional staff throughout Latin America
and the Caribbean and from the Ministries of Health of selected
countries. These experts possess a wide variety of technical skills:
health services administration, medicine, general management,
mental health, sanitary engineering, logistics, coordination,
water and sanitation, epidemiology, damage and needs assessment,
information and communications and toxicology.
For some time PAHO has maintained a small electronic Roster
of health experts to identify candidates with a particular disaster-related
skill set. Now, with the formal creation of the Health Disaster
Response Team, the redesign of the Roster is almost complete.
This will permit PAHO/WHO to centralize data on team members and
rapidly select and contact individuals for deployment.
Training workshops for team members have taken place in the
Dominican Republic and Costa Rica to update and streamline the
Organization’s internal administrative procedures (to increase
flexibility in emergency situations) and to foster teamwork among
experts, most of whom share a common organizational affiliation
but who previously had little opportunity to work together. The
workshops focused on improving emergency-related skills including:
the coordination of humanitarian supplies in the aftermath of
disasters; conducting damage assessments; resource mobilization;
developing recovery and rehabilitation plans and communications
and information management. The agenda for the February training
session in Costa Rica is attached as Annex
11.
Manual
and Guidelines
The first draft of a Disaster Response Team Manual was written,
translated from Spanish to English, and reviewed by several experts
in the Region. The manual will be a living document and will be
revised following a major disaster in orderto incorporate missing
or other required information and to revise procedures. User-friendly
web-based and print versions are being prepared. The manual will
also be available on CDROM and will be widely distributed among
team members and PAHO offices. Many of the Organization’s
internal administrative arrangements are being updated and reference
to these is included in the Response Team Manual. This manual,
parts of which are interactive, is housed on PAHO/WHO’s
Intranet site. A print version of the manual is available on request.
Equipment
and Supplies
Experience following the December 2004 tsunami in south Asia
helped the World Health Organization to develop the content of
a “Survival Kit for One Person.” Using this list as
a guide, PAHO purchased and assembled 15 basic survival kits and
pre-positioned them in the three subregional disaster offices:
Barbados (for the Caribbean), Panama (for Central America) and
Ecuador (for South America). The utility of these kits will be
tested at the first opportunity and their content will be reevaluated.
The pre-positioning of the equipment and supplies will at least
facilitate the deployment of the team to an affected area. In
the case of hurricanes, the pre-positioning of a team will be
decided according to the each individual situation.
In summary, the makeup of the team is multidisciplinary and members
have substantial experience in their area of expertise. All are
now much more familiar with internal PAHO/WHO procedures and can
therefore speed up the response by cutting through red tape. The
creation of this Team and the inter-programmatic support it receives
is an important indicator of the fact that humanitarian response
to disasters in PAHO Member States is a collective responsibility
of the entire Organization.
The United Nations humanitarian reform and the creation of the
cluster mechanism have played a role in how PAHO/WHO has organized
this team and selected members. In disaster situations, the Team
Coordinator will also serve as the health cluster lead and will
be tasked with liaising with all other agencies. In Colombia and
Haiti, countries which are in complex emergencies, a system is
already in place and PAHO/WHO is coordinating health issues. Read
PAHO’s newsletter editorials on the UN Cluster Approach
in Annex 12.
The Logistics Support
System
 The
LSS is a joint initiative of six UN agencies (WHO, WFP, OCHA,
UNICEF, UNHCR, and PAHO) to consolidate the experiences of the
UN Joint Logistics Centre (UNJLC) and the SUMA system in the Americas
with regard to the management of humanitarian supplies. LSS combines
the strengths of these two successful initiatives that have operated
in different environments and have served complementary purposes.
The
LSS is a joint initiative of six UN agencies (WHO, WFP, OCHA,
UNICEF, UNHCR, and PAHO) to consolidate the experiences of the
UN Joint Logistics Centre (UNJLC) and the SUMA system in the Americas
with regard to the management of humanitarian supplies. LSS combines
the strengths of these two successful initiatives that have operated
in different environments and have served complementary purposes.
The English and Spanish-language versions of the LSS software
were finalized in 2006 and widely tested. LSS has its own web
site www.lssweb.net
where the software can be downloaded free of charge. The web site
is also regularly updated with LSS activities and operations (in
English and Spanish), a team of LSS members was formed and its
members incorporated into the PED roster, the LSS was implemented
in several locations following different disasters (floods in
Colombia and Suriname, crisis in Lebanon), and a CD-Rom containing
the LSS software, manuals in both languages, instructions for
setting up the web application, PowerPoint presentation and other
information was developed and is being distributed free of charge.
 There
was good reception of LSS in all the countries were training activities
took place and there is even a request to translate it into Turkish
after the training in Ankara. During 2007, it is expected that
the software and manuals will be translated into French and Portuguese,
so all PAHO member countries will be able to use the system in
their national language. The availability of the French version
will also facilitate its dissemination to other regions.
There
was good reception of LSS in all the countries were training activities
took place and there is even a request to translate it into Turkish
after the training in Ankara. During 2007, it is expected that
the software and manuals will be translated into French and Portuguese,
so all PAHO member countries will be able to use the system in
their national language. The availability of the French version
will also facilitate its dissemination to other regions.
Meetings are held with NGOs, UN agencies and National Authorities
of each country where the LSS is deployed or training take place.
These meetings emphasize the importance of accountability and
transparency in the management of humanitarian aid. The objective
of promoting good governance is far more ambitious and perhaps
important that the improvement of the software and its utilization
as an inventory control tool. However, contribution to coordination
and transparency will only be fully accomplished if a culture
of collaboration and frank exchange of data among international
agencies and national partners exists. The shortcomings are generally
not software or system problems but a lack of willing to share
data and lack of political support.