2. Disaster Mitigation
It is estimated that more than half of the hospitals in Latin
America and the Caribbean are located in disaster-prone areas,
which makes them unsafe. This situation is not specific to this
Region; the tsunami and earthquakes in India (Gujarat), Iran (Bam),
and Pakistan also severely affected health infrastructure. Building
codes for health facilities should not only ensure the survival
of staff and patients but also be stringent enough to permit facilities
to continue functioning.
The destruction of Mexico’s Hospital Juarez in 1985, which
resulted in the death of 561 patients and staff, prompted the
Region to launch a massive awareness campaign to increase the
structural and nonstructural safety of health facilities. This
concern, at first a regional issue, evolved into a global priority
in January 2005, when the “Hyogo Framework of Action for
2005-2015,” the global blueprint stemming from the Second
World Conference on Disaster Reduction held in Kobe, Japan, included
a specific indicator on vulnerability reduction in the health
sector.
When PAHO/WHO speaks about disaster mitigation it focuses on
how the health sector can reduce the physical and functional vulnerability
of all types and levels of health facilities. At the regional
and national level, PAHO advocates for and collaborates with Ministries
of Health and Planning, financial lending institutions, professional
associations and others to establish regulatory agreements that
contribute to making hospitals safe in disaster situations.
Safe Hospitals
 The
goal of “hospitals safe from disaster,” which was
approved by 168 countries worldwide at the 2005 Kobe Conference,
complements PAHO/WHO’s commitment to the importance of building
new hospitals with a level of protection that guarantees they
can remain operational after a disaster. This commitment also
extends to applying risk-reduction mitigation measures in existing
facilities to reduce their
The
goal of “hospitals safe from disaster,” which was
approved by 168 countries worldwide at the 2005 Kobe Conference,
complements PAHO/WHO’s commitment to the importance of building
new hospitals with a level of protection that guarantees they
can remain operational after a disaster. This commitment also
extends to applying risk-reduction mitigation measures in existing
facilities to reduce their
vulnerability. To assist in making strides in this field, PAHO
advocates for and collaborates with national authorities in the
Region to develop tools, policies and regulatory agreements as
well as to provide training for engineers, building inspectors
and project managers.
One of the most important advances in 2006 was the development
of a Hospital Safety Index, a tool or scorecard that measures
and ranks a health facility’s level of safety in the context
of its geographical location and exposure to natural hazards.
As not all hospitals face the same risks, nor are they built using
the same standards, this model incorporates a wide range of factors
that measure safety. To reach a final safety score, hospitals
must look at factors such as where the hospital is built (i.e.,
is it in an earthquake-prone area?), the structure of the building,
its configuration, construction materials used, and its previous
exposure to hazards. Attention is also given to non-structural
hospital components such as the electric system, water supply
and reservoir, ventilation, furniture, medical equipment, etc.
The final section of the Hospital Safety Index evaluates the organization
of the facility, the existence and application of an emergency
plan and the level of awareness of staff. The DiMAG, the Disaster
Mitigation Advisory Group, prepared the first draft of this scorecard,
which can be used by engineers, hospital directors and disaster
managers and takes very little time to apply. However it does
not replace an in-depth vulnerability assessment conducted by
experienced engineers. And, having a tool to assess safety, with
a focus on critical services, does not automatically mean that
recommended measures will be taken to improve the situation. The
Hospital Safety Index form is attached in Annex
8.
 Mexico
and, to a more limited degree St. Vincent, Dominica Cuba, Peru
and Costa Rica, conducted pilot surveys to test the Hospital Safety
Index. The application of the Safety Index in Mexico, a large
country with more than 3,000 public and private hospitals, offered
an interesting example of how this process works. In 2006, Mexico
created a National Committee for the Diagnosis and Certi fication
of Safe Hospitals, made up of representatives of a variety of
institutions such as the Mexican Hospital Association, the Social
Security Institute and the Secretary of Health, among others.
The Committee helped to pilot the application of the Hospital
Safety Index in more than 100 Mexican health facilities which
were determined to be at risk, either because of their geographic
location or due to their critical place in the health network.
Mexico
and, to a more limited degree St. Vincent, Dominica Cuba, Peru
and Costa Rica, conducted pilot surveys to test the Hospital Safety
Index. The application of the Safety Index in Mexico, a large
country with more than 3,000 public and private hospitals, offered
an interesting example of how this process works. In 2006, Mexico
created a National Committee for the Diagnosis and Certi fication
of Safe Hospitals, made up of representatives of a variety of
institutions such as the Mexican Hospital Association, the Social
Security Institute and the Secretary of Health, among others.
The Committee helped to pilot the application of the Hospital
Safety Index in more than 100 Mexican health facilities which
were determined to be at risk, either because of their geographic
location or due to their critical place in the health network.
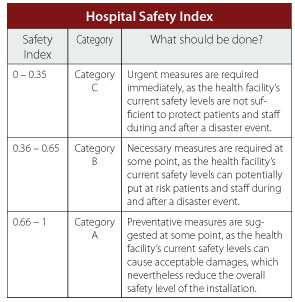
 As
a first step, more than 60 professionals were trained to use this
tool, which classifies the level of safety in hospitals into categories
A, B or C (see box). The Index was then applied in 104 health
facilities by the end of November 2006. The results showed that
more than 60% of these hospitals were classified as safe in terms
of structural and non-structural components. However, almost the
same percentage were deemed to require improvement in the functional
component (disaster planning, organization, training, critical
resources, etc.) After reviewing the results, Mexico’s coordinator
of the Civil Protection system committed to include “Safe
Hospitals” as a national disaster reduction priority, for
which he received the backing of the country’s newly-elected
president. Mexico is committed to applying the hospital safety
index to all high-risk facilities (slightly over 1,000) in 2007
and to begin the process of certifying those facilities with an
“A” rating. The results of this pilot project are
attached in a presentation in Annex 9.
As
a first step, more than 60 professionals were trained to use this
tool, which classifies the level of safety in hospitals into categories
A, B or C (see box). The Index was then applied in 104 health
facilities by the end of November 2006. The results showed that
more than 60% of these hospitals were classified as safe in terms
of structural and non-structural components. However, almost the
same percentage were deemed to require improvement in the functional
component (disaster planning, organization, training, critical
resources, etc.) After reviewing the results, Mexico’s coordinator
of the Civil Protection system committed to include “Safe
Hospitals” as a national disaster reduction priority, for
which he received the backing of the country’s newly-elected
president. Mexico is committed to applying the hospital safety
index to all high-risk facilities (slightly over 1,000) in 2007
and to begin the process of certifying those facilities with an
“A” rating. The results of this pilot project are
attached in a presentation in Annex 9.
In the Caribbean—where a single hospital can be of vital
importance, as it may be the only one in a country—additional
considerations have been added to the form to measure the degree
of disruption to a health facility if the recommendations are
implemented and the cost associated with doing so. Authorities
can appreciate at a glance that with limited funds and minor disruption,
their safety score can be improved. The box below, shows a sample
of this expanded form.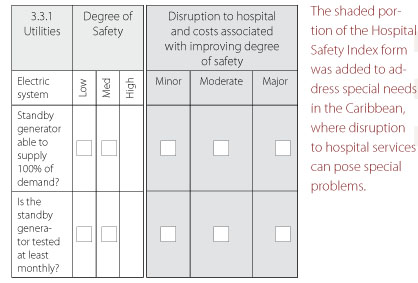
Most countries in which the Hospital Safety Index was piloted
were very cooperative and enthusiastic about applying it. However,
for understandable reasons, health authorities or ministries of
health requested that the results be kept confidential!
Countries Take Steps to Protect their
Health Facilities
In Costa Rica,
the impact of the 2005 fire that destroyed part of the Calderon
Guardia Hospital in Costa Rica, killing 19 patients and staff,
was not only measured in economic terms but also in the social
and political repercussions it left in its wake. The painful realization
of the vulnerability of health care facilities to manmade as well
as natural disasters prompted the directors of Costa Rica’s
Social Security System (CCSS), which is responsible for and the
only provider of the nation’s hospital services, to prepare
a policy to safeguard the country’s health services. PAHO/WHO
supported the government and a multidisciplinary team, which they
created to develop this policy. The result was a proposal for
an institutional policy on Hospital Safety that identified the
steps necessary to transform a policy “on paper” into
a reality.
In order to create a national committee to develop a safe hospital
policy, the CCSS had to formally modify its organizational structure.
The policy which was created focused on investments in new facilities,
existing facilities and on preparedness actions to protect the
lives of patients and staff. A number of intersectorial measures
were put in place to monitor compliance with this policy. Technical
reference material on a model national program for safe hospitals,
which PAHO/WHO helped to develop during earlier efforts with other
countries in the Region, was used in Costa Rica.
Costa Rica’s safe hospital policy set forth deadlines,
allotted funds for activities and assigned responsibilities. Once
this work was completed, the policy was presented to the board
of directors of the CCSS, which approved it through a formal resolution.
To begin implementation of the policy in Costa Rica’s health
facilities, the CCSS assigned US$3 million of its own funds. More
concretely, in the design of the new Heredia Hospital, vulnerability
reduction measures were included; particularly noteworthy were
measures designed for fire safety, a tangible legacy of the tragic
Calderon Guardia fire.
Paraguay’s
Ministry of Public Heath and Social Welfare also demonstrated
a commitment to protecting the country’s health facilities.
The Minister of Health, in a letter to PAHO/WHO, requested assistance
in assuming responsibility for carrying out a Safe Hospitals program
to complement parallel activities aimed at achieving the Millennium
Development Goals. It is important to note that the political
support from a country’s highest level health official is
key to the success of efforts in this field. Specifically, the
Ministry sought help in the form of technical experts to carry
out an evaluation of the vulnerability of the Ministry’s
health facilities to disasters, to arm the country with the information
necessary to develop projects and strategies within the framework
of Safe Hospitals.
In Argentina,
the Ministry of Health, with the support of PAHO, organized a
250-person meeting on Safe Hospitals for the Province of Buenos
Aires. The meeting was held to raise awareness among hospital
directors, maintenance supervisors, municipal health leaders and
deans of faculties of medicine, engineering and architecture of
the importance of reducing vulnerability in health facilities.
The Ministry of Health proposed several lines of action for safeguarding
provincial hospitals, including passing a legal framework to regulate
the construction of new health facilities, conducting vulnerability
assessments in existing structures, promoting specialized training
in architecture and engineering and earmarking 30% of the Ministry’s
annual budget for infrastructure for maintenance and safety of
hospitals.
Protecting Health Facilities: Who is
in charge?
There is a general agreement that in order to protect health
facilities and reach the goal of safe hospitals, key actors outside
the health sector must be involved. Unfortunately, this premise
is still not clear in many countries. Peru went through a sometimes
complex and challenging process at the national decision making
level to answer the basic question: who is in charge of protecting
health facilities?
The Peruvian Civil Defense Institute, as part of its routine
activities in public and private facilities, decided to conduct
a safety inspection of the main hospital in Cajamarca, a city
in northern Peru. The results of the evaluation showed that the
hospital indeed required significant improvements in areas that
were outlined in the safety norms of the national Civil Defense.
While the issues arising from the findings of the evaluation were
resolved, the hospital might have to be closed. This internal
report was leaked to the media by local authorities, and quickly
the Minister of Health denied the Civil Defense the right to inspect
hospitals; the Minister went further and asked for the resignation
of the head of the Civil Defense because of interference in the
health sector. There was concern that if inspections were performed
in other hospitals, the results might be similar and this would
have an adverse political and social impact.
PAHO/WHO helped both institutions to resolve this impasse, recognizing
the authority of the Civil Defense to evaluate all public and
private facilities, but at the same time, indicating that hospitals
cannot be evaluated in the same way as schools, shopping centers,
restaurants or other public places. The Ministry of Health and
the Civil Defense agreed to work together, with the technical
support of PAHO, to prepare technical guidelines to assess hospital
safety, to train safety inspectors in health facilities and to
identify and improve the safety of health facilities that are
found to be unsafe according to the new guidelines.
Reaching common ground proved to be in the best interest of
the Peru’s public and private facilities. The Civil Defense
offered to finance the evaluation of the first two hospitals,
using public disaster mitigation funds. The new guidelines for
hospital safety assessment, prepared with the support of the Peru-Japan
Center for Earthquake Engineering Research and Disaster Mitigation,
were officially approved by the Government of Peru, becoming the
first national norm of its kind in the Americas. Peru is now training
and accrediting hospital safety inspectors and will soon begin
the assessment of public and private health facilities countrywide.
Advocacy and Awareness
By the end of 2006, it had been decided that the focus of the
2008-09 World Disaster Reduction Campaign of the International
Strategy for Disaster Reduction (ISDR) would be on reducing the
risks of natural hazards on the health of people worldwide. This
decision provided an excellent opportunity for PAHO/WHO to use
this global forum as a platform to further promote a risk reduction
and mitigation strategy in this Region, under the banner of Safe
Hospitals. Because of the Organization’s substantial experience
and achievements in this field, the ISDR has reached out to PAHO/WHO
for technical and advocacy support as the campaign develops. Although
work will begin in earnest in 2007, PAHO/WHO proposes that global
focus be on ensuring the structural resilience of health facilities
to protect the lives of the patients and staff, the functional
continuity of hospitals and key health services in the aftermath
of disasters, when they are most needed. The campaign will provide
an excellent chance to engage the public and decision makers in
all sectors as stakeholders in the safety of their country’s
hospitals.
A new DVD program on Safe Hospitals
has been prepared to raise awareness and promote the concept and
strategy, with a perspective that extends beyond the health sector.
The video explains what a safe hospital is and why we must safeguard
these critical facilities. It highlights examples of good practices
in the Region, destroying the myth that it would be too expensive
or even impossible to build hospitals with safeguards to ensure
they continue to function after disasters. The DVD combines video
footage and interviews with important decision makers in several
countries in the Americas who share positive experiences and lobby
for safe hospitals. The program is geared toward the political
arena to raise awareness at the decision- making level during
planning or execution of hospital construction or improvements.
However, it is equally as suitable for use in disaster mitigation
training activities. In addition to serving as an excellent reference
source, this type of program will become key to PAHO’s advocacy
efforts in conjunction with the ISDR global campaign and offer
an example to other regions of the world wishing to create similar
products.